Is there a difference between natural and synthetic cannabinoids?
In principle exact copies of naturally occurring cannabinoids can be synthesized. Therefore, synthetic cannabinoids are not necessarily different from natural cannabinoids. However, in practice synthetic cannabinoids are produced to be more specific and more powerful than natural cannabinoids, which can have a dramatic effect on their safety profile.
Entourage effect
Although exact copies of natural cannabinoids can be synthesized, natural cannabinoids from plants or extracts are flanked by numerous other compounds such as other cannabinoids or terpenes whereas synthetic cannabinoids usually are not.
Like the main ingredient / the cannabinoid of interest, these other compounds also bind one or more cannabinoid receptors and will therefore alter the effect that the cannabinoid of interest has.
Although it is not exactly known how this so called ‘entourage effect’ works, it is known that it consistently improves the therapeutic potential of cannabinoids (Gallily et al., 2015; Russo, 2011; Russo and Guy, 2006).
Specificity
Natural cannabinoids typically bind to more than one receptor and therefore exert more than one effect. While this ‘promiscuity’ of natural cannabinoids may be very useful in normal physiology this can frustrate research attempting to elucidate the exact mechanism behind a disease or a therapy. Therefore, for research purposes, synthetic compounds / cannabinoids that are highly specific for a particular receptor can be very useful. For instance mapping the distribution of CB1 receptors can only be done faithfully when the used probe is highly specific for CB1 and does not cross-react with any other receptor in the body (Ceccarini et al., 2015).
Efficacy
Natural cannabinoids typically are gentle modulators of receptor activity that have a moderate affinity for their receptor that is short-lasting and can be washed away by other compounds / modulators. Synthetic cannabinoids are often designed to have a high affinity for their receptor and have a lasting effect.
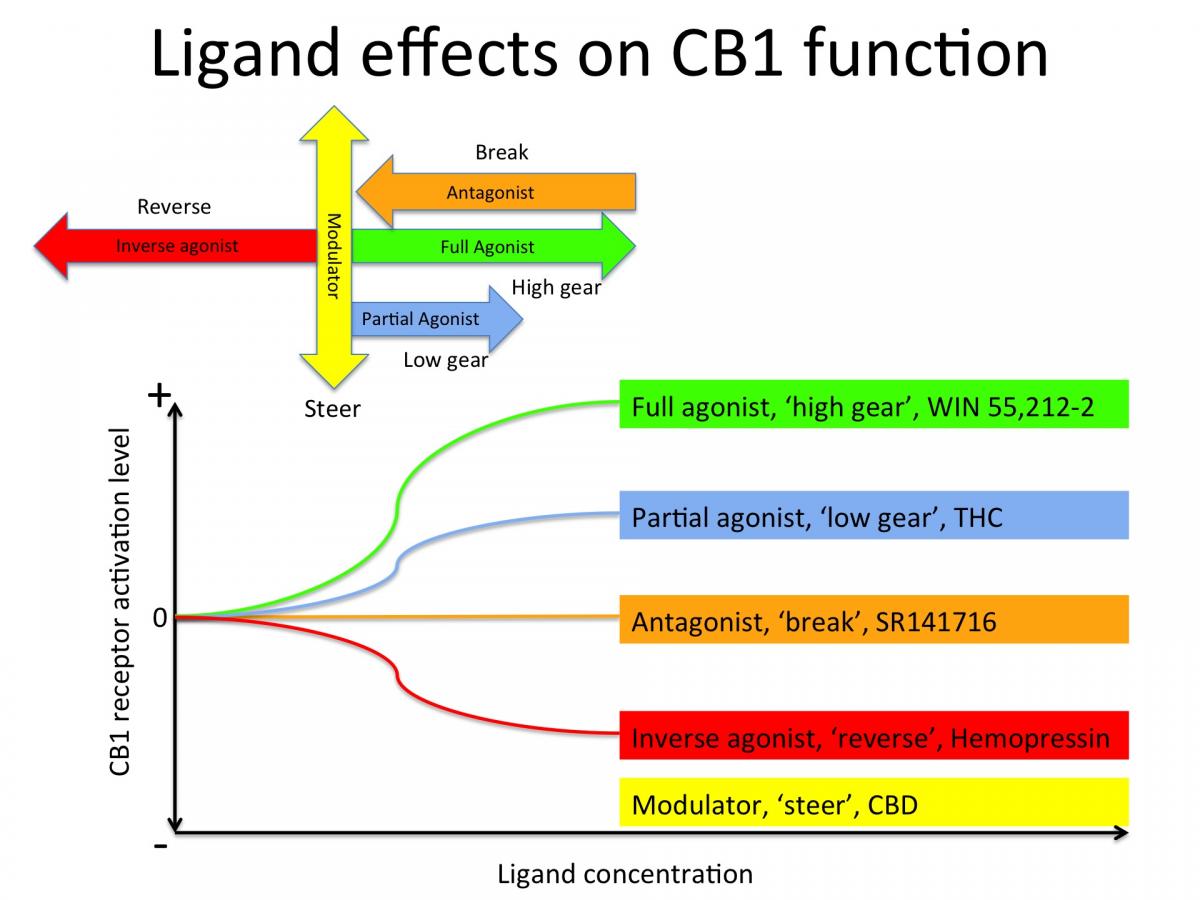
THC for example is a partial agonist for CB1. If CB1 were a car engine, THC would put it in first gear. It’s synthetic analogue, Win55212-2 is a full agonist, which would put CB1 in high gear with a brick on the accelerator. SR141716 is a synthetic CB1 antagonist, which would slam on the break and bring the CB1 engine to a full stop. CBD does not seem to bind directly to the activation site of CB1 but to other parts of the receptor, thereby modulating or 'steering' the function of CB1 (see figure below).
Safety
Although synthetic cannabinoids can be very useful in basic research to elucidate molecular mechanisms in physiological processes, they can be dangerous if not lethal in clinical use / humans. For instance, rimonabant / SR141716 was introduced as an anti-obesity drug but subsequently pulled of the market for its potential to trigger serious psychiatric side effects or even suicide. With the advent of both recreational and medicinal cannabis the market is increasingly flooded with synthetic cannabinoids. This is at least partially due to the fact that synthetic compounds can be patented and therefore more profitable than natural cannabinoids. As a result serious injuries and even fatalities due to synthetic cannabinoid use are now reported almost on a daily basis (Adedinsewo et al., 2016; van Amsterdam et al., 2015; Babi et al., 2017; Barceló et al., 2017; Buyukbese Sarsu, 2016; Cha et al., 2015; Clark et al., 2015; Degirmenci et al., 2015; Demir et al., 2017; Efe et al., 2017; Ezaki et al., 2016; FuNADA and Takebayashi-Ohsawa, 2017; Karass et al., 2017; Kırgız and Kaldırım, 2017; Kusano et al., 2017; Mansoor et al., 2017; McIlroy et al., 2016; Moeller et al., 2017; Monte et al., 2017; Öcal et al., 2016; Ozturk et al., 2017; Raheemullah and Laurence, 2016; Samra et al., 2017; Shanks and Behonick, 2016; Waugh et al., 2016; Zarifi and Vyas, 2017).
Natural cannabis / cannabinoids has been used around the world for over 6.000 years without a single reported fatality and are thus far, far safer than synthetic cannabinoids.
References:
Adedinsewo, D.A., Odewole, O., and Todd, T. (2016). Acute Rhabdomyolysis Following Synthetic cannabinoid Ingestion. North Am. J. Med. Sci. 8, 256–258.
van Amsterdam, J., Brunt, T., and van den Brink, W. (2015). The adverse health effects of synthetic cannabinoids with emphasis on psychosis-like effects. J. Psychopharmacol. Oxf. Engl.
Babi, M.-A., Robinson, C.P., and Maciel, C.B. (2017). A spicy status: Synthetic cannabinoid (spice) use and new-onset refractory status epilepticus-A case report and review of the literature. SAGE Open Med. Case Rep. 5, 2050313X17745206.
Barceló, B., Pichini, S., López-Corominas, V., Gomila, I., Yates, C., Busardò, F.P., and Pellegrini, M. (2017). Acute intoxication caused by synthetic cannabinoids 5F-ADB and MMB-2201: A case series. Forensic Sci. Int. 273, e10–e14.
Buyukbese Sarsu, S. (2016). Unusual side effect of cannabis use: acute abdomen due to duodenal perforation. Int. J. Emerg. Med. 9, 18.
Ceccarini, J., Kuepper, R., Kemels, D., van Os, J., Henquet, C., and Van Laere, K. (2015). [18F]MK-9470 PET measurement of cannabinoid CB1 receptor availability in chronic cannabis users. Addict. Biol. 20, 357–367.
Cha, H.J., Seong, Y.-H., Song, M.-J., Jeong, H.-S., Shin, J., Yun, J., Han, K., Kim, Y.-H., Kang, H., and Kim, H.S. (2015). Neurotoxicity of Synthetic cannabinoids JWH-081 and JWH-210. Biomol. Ther. 23, 597–603.
Clark, B.C., Georgekutty, J., and Berul, C.I. (2015). Myocardial Ischemia Secondary to Synthetic cannabinoid (K2) Use in Pediatric Patients. J. Pediatr.
Degirmenci, Y., Kececi, H., and Olmez, N. (2015). A case of ischemic stroke after bonzai: syntetic cannabinoid from Turkey. Neurol. Sci. Off. J. Ital. Neurol. Soc. Ital. Soc. Clin. Neurophysiol.
Demir, T., Onan, H.B., Salkin, F.O., and Bicakci, S. (2017). Distal internal carotid artery dissection after consumption of synthetic cannabinoid “Bonzai.” Neurol. Neurochir. Pol.
Efe, T.H., Felekoglu, M.A., Çimen, T., and Doğan, M. (2017). Atrial fibrillation following synthetic cannabinoid abuse. Turk Kardiyol. Dernegi Arsivi Turk Kardiyol. Derneginin Yayin Organidir 45, 362–364.
Ezaki, J., Ro, A., Hasegawa, M., and Kibayashi, K. (2016). Fatal overdose from synthetic cannabinoids and cathinones in Japan: demographics and autopsy findings. Am. J. Drug Alcohol Abuse 1–10.
FuNADA, M., and Takebayashi-Ohsawa, M. (2017). Synthetic cannabinoid AM2201 induces seizures: Involvement of cannabinoid CB1 receptors and glutamatergic transmission. Toxicol. Appl. Pharmacol. 338, 1–8.
Gallily, R., Yekhtin, Z., and Hanuš, L.O. (2015). Overcoming the Bell-Shaped Dose-Response of Cannabidiol by Using Cannabis Extract Enriched in Cannabidiol. Pharmacol. Amp Pharm. 06, 75.
Karass, M., Chugh, S., Andries, G., Mamorska-Dyga, A., Nelson, J.C., and Chander, P.N. (2017). Thrombotic microangiopathy associated with synthetic cannabinoid receptor agonists. Stem Cell Investig. 4, 43.
Kırgız, A., and Kaldırım, H. (2017). Bilateral multiple exudative retinal detachments and macular edema in a patient diagnosed with synthetic cannabinoid (Bonzai) intoxication. Int. Ophthalmol.
Kusano, M., Zaitsua, K., Taki, K., Hisatsune, K., Nakajima, J., Moriyasu, T., Asano, T., Hayashi, Y., Tsuchihashi, H., and Ishii, A. (2017). Fatal Intoxication by 5F-ADB and Diphenidine: Detection, Quantification, and Investigation of their Main Metabolic Pathways in Human by LC/MS/MS and LC/Q-TOFMS. Drug Test. Anal.
Mansoor, K., Zawodniak, A., Nadasdy, T., and Khitan, Z.J. (2017). Bilateral renal cortical necrosis associated with smoking synthetic cannabinoids. World J. Clin. Cases 5, 234–237.
McIlroy, G., Ford, L., and Khan, J.M. (2016). Acute myocardial infarction, associated with the use of a synthetic adamantyl-cannabinoid: a case report. BMC Pharmacol. Toxicol. 17, 2.
Moeller, S., Lücke, C., Struffert, T., Schwarze, B., Gerner, S.T., Schwab, S., Köhrmann, M., Machold, K., Philipsen, A., and Müller, H.H. (2017). Ischemic stroke associated with the use of a synthetic cannabinoid (spice). Asian J. Psychiatry 25, 127–130.
Monte, A.A., Calello, D.P., Gerona, R.R., Hamad, E., Campleman, S.L., Brent, J., Wax, P., Carlson, R.G., and ACMT Toxicology Investigators Consortium (ToxIC) (2017). Characteristics and Treatment of Patients with Clinical Illness Due to Synthetic cannabinoid Inhalation Reported by Medical Toxicologists: A ToxIC Database Study. J. Med. Toxicol. Off. J. Am. Coll. Med. Toxicol.
Öcal, N., Doğan, D., Çiçek, A.F., Yücel, O., and Tozkoparan, E. (2016). Acute Eosinophilic Pneumonia with Respiratory Failure Induced by Synthetic cannabinoid Inhalation. Balk. Med. J. 33, 688–690.
Ozturk, H.M., Erdogan, M., Alsancak, Y., Yarlioglues, M., Duran, M., Boztas, M.H., Murat, S.N., and Ozturk, S. (2017). Electrocardiographic alterations in patients consuming synthetic cannabinoids. J. Psychopharmacol. Oxf. Engl. 269881117736918.
Raheemullah, A., and Laurence, T.N. (2016). Repeated Thrombosis After Synthetic cannabinoid Use. J. Emerg. Med.
Russo, E.B. (2011). Taming THC: potential cannabis synergy and phytocannabinoid-terpenoid entourage effects. Br. J. Pharmacol. 163, 1344–1364.
Russo, E., and Guy, G.W. (2006). A tale of two cannabinoids: the therapeutic rationale for combining tetrahydrocannabinol and cannabidiol. Med. Hypotheses 66, 234–246.
Samra, K., Boon, I.S., Packer, G., and Jacob, S. (2017). Lethal high: acute disseminated encephalomyelitis (ADEM) triggered by toxic effect of synthetic cannabinoid black mamba. BMJ Case Rep. 2017.
Shanks, K.G., and Behonick, G.S. (2016). Death after use of the synthetic cannabinoid 5F-AMB. Forensic Sci. Int.
Waugh, J., Najafi, J., Hawkins, L., Hill, S.L., Eddleston, M., Vale, J.A., Thompson, J.P., and Thomas, S.H.L. (2016). Epidemiology and clinical features of toxicity following recreational use of synthetic cannabinoid receptor agonists: a report from the United Kingdom national poisons information service. Clin. Toxicol. Phila. Pa 1–7.
Zarifi, C., and Vyas, S. (2017). Spice-y Kidney Failure: A Case Report and Systematic Review of Acute Kidney Injury Attributable to the Use of Synthetic Cannabis. Perm. J. 21.